September/October Issue of vein specialist
Venous Disease Ever Upward
Emerging Technology
Table of Contents
Message from the Editor
Steve Elias, MD
Emerging Technologies
Simplifying DVT Diagnosis by Non-experts using AI-assisted Ultrasonography
Makis Avgerinos, MD
Amsel’s SCureClamp™ and InVera: Disruptive Medical Devices
Lowell Kabnick, MD
Unlocking Consistency in Sclerotherapy: The Impact of VARIXIO Technology
Adam M. Gwozdz, MD, MSc
On the Move with Koya’s Dayspring Non-pneumatic Compression Device (NPCD)
Thomas S. Maldonado, MD
AI Puts Member Engagement in Overdrive
Sherry Budziak
Interview with ChatGPT
Eric Hager, MD
Membership Matters
JVS-VL Going Open Access: What does it mean?
Ruth Bush, MD and Anil Hingorani, MD
For the Love of the Game
Gary Burnison
JVS-VL Welcomes New Social Media Editor
Welcome New Members
July/August
Copyright © 2023 by The American Venous Forum. All rights reserved.
EDITOR-IN-CHIEF
Steve Elias, MD
EXECUTIVE EDITOR
John Forbes, MBA
MANAGING EDITOR
Allie Woodward
PUBLICATION DESIGNER
Anthony Eaves
Message from the Editor

Steve Elias, MD
Editor-in-Chief, Vein Specialist
The Neighborhood
We all have neighbors–whether you live in the city, the suburbs, or the middle of Montana. You may know all of them, some of them, or none of them; but you share a commonality of geography. You may speak with them a lot, a little, or never. I have a neighbor who walks her dog, a labradoodle, constantly. And when she walks him, she is always on the phone, old school. No headphones, no Airpods. Just hand-held to the ear. I have not had more than a 2-word conversation with her, yet she is speaking with others constantly and continuously. Am I jealous? No. I have nothing to say to this person. Still I wonder, who is she always speaking to? Or is she? My daughter thinks it is all an act. An act of conversation. She really isn’t talking to anyone. If ostensibly you are on the phone, you don’t need to engage with anyone you encounter. Coward. Don’t fake the phone conversation when you’re walking in the neighborhood. Don’t hide. Be Mr Rogers;embrace your neighborhood.
Just like we embrace all of our venous neighbors in each issue of Vein Specialist. Moving ever upward. This issue is about the new, the emerging technologies and concepts in venous disease. A few things about AI and its expanding use. Makis Avgerinos discusses AI’s use to allow non-experts to diagnose acute DVT all over the world. Just requires a phone. Eric Hager lets us know where ChatGPT may fit in. AI can also be used for membership issues as Sherry Budziak writes. Emerging technologies we include: SCureClamp™ and Invera (Lowell Kabnik), VARIXIO® (Adam Gwozdz), and the Dayspring Compression device (Tom Maldonado). As AVF continues its rise ever upward in the vein world, membership matters. We introduce new members and the new Journal of Vascular Surgery—Venous and Lymphatic Disorders Social Media Editor. An organization is only as good as its members. This is no mystery.
But there are other mysteries aside from the mystery of who is my neighbor talking to. A childhood mystery: “Who stole the cookie from the cookie jar?” Do they even still sell cookie jars? Well, they didn’t in England in the 18th Century, but they did sell cookie tins back then. This is when the game began, but the words were: “Who took the biscuit from the biscuit tin?” They don’t sell many biscuit tins anymore. The modern version of the game had a change in popularity during the Great Depression when ceramic jars contained things: spare change, candy, and cookies. The moniker “Great Depression” implies there must have been a “Not-So-Great Depression.” Was there ever? I don’t think so, but the Great Depression persists in our collective unconscious, as Carl Jung explained. Meanwhile, if you ever played “Who stole the cookie from the cookie jar,” you never find the answer. It is, as Wikipedia says, infinitely recursive. Never ending. But this issue of Vein Specialist ends with 2 mysteries unsolved: Who is my neighbor speaking to and who stole the cookie from the cookie jar? If you know the answers, please let me know. It is hard to sleep at night. These uncertainties persist, but not the uncertainty of what’s new in the vein neighborhood. We got that covered.

Simplifying DVT Diagnosis by Non-experts using AI-assisted Ultrasonography

Efthymios Avgerinos, MD
Professor of Vascular Surgery
Athens Medical Center, University of Athens
Deep venous thrombosis (DVT) and associated pulmonary embolism (PE) are highly prevalent both in the US and Europe, occurring in 1–2 per 1000 individuals each year. In the US, the total numbers exceed one million events per year. Given that 20% of patients with PE die within one year of presentation and 20-30% will develop post-thrombotic morbidity, diagnosing and treating DVT in a timely fashion is of utmost importance.
Diagnostic algorithms for leg DVT typically require a combination of clinical probability test assessment, a standard lower leg duplex, or, at a minimum, 2-point compression ultrasound (sometimes bilateral) and d-dimer testing. A DVT duplex is the most frequently requested vascular ultrasound study and in the vast majority (~90%), it is negative. These studies can be costly and time consuming both for patients and physicians in an otherwise busy emergency room or vascular ultrasound lab. Maintaining expert sonographers or radiologists on-call after hours increases costs further and exposes them to fatigue and burnout. Vascular lab- or radiology-performed DVT studies are otherwise not universally available, which delays diagnosis. Point-of-care compression ultrasound (POCUS) is increasingly used by emergency physicians, but despite quality evidence and recommendations, it is not used widely and it may share common logistical difficulties with standard duplex.
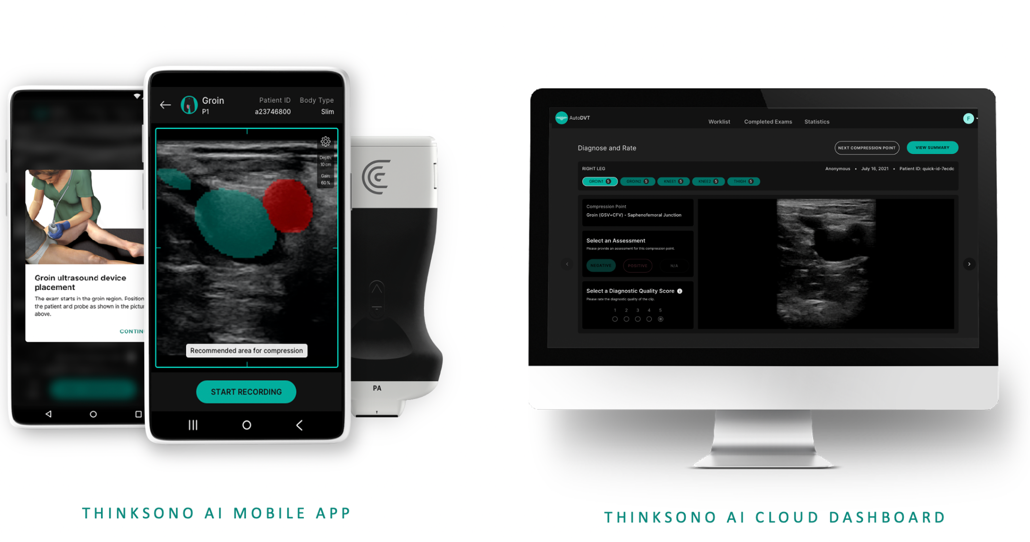
Artificial intelligence (AI) has proven to recognize complicated scan patterns and provide quantitative and qualitative assessments for imaging data. AutoDVT (www.thinksono.com), a machine-learning software, is an AI tool that guides non-specialists in acquiring appropriate 2-point (common femoral and popliteal veins) compression sequences. A smartphone or tablet and a wireless ultrasound probe are the only equipment needed. The captured images are then uploaded to the cloud and remotely reviewed by an expert. (Figure) Simply, a nurse or non-expert physician can be guided by the AI software to perform a DVT POCUS. Then the images are evaluated by the expert on their cellphone or computer as diagnostic or non-diagnostic for DVT. The software is trained to make its own diagnosis —which it does very accurately. The more images we feed the software, the higher its diagnostic accuracy will be when we allow it to suggest a diagnosis.
With the first European trials enrolling >500 patients now complete, US studies and FDA clearance are underway. Preliminary comparative studies of AutoDVT against standard duplex yielded a sensitivity of 100% and a specificity of 95.12%, (PPV 75%, NPV 100%), sparing the need of the duplex in 53% of emergency room cases suspicious for DVT.
AutoDVT has the potential to revolutionize DVT diagnosis in several clinical settings and scenarios beyond the emergency room (eg, remote environments without radiology services, critically ill patients, post saphenous ablation), reducing the need and cost of multiple unnecessary duplex scans. Radiologist and sonographer resources can be reallocated, patient waiting times can be reduced, and lives can be changed.
FIGURE 1
References
- Kainz B, Heinrich MP, Makropoulos A, et al. Non-invasive diagnosis of deep vein thrombosis from ultrasound imaging with machine learning. NPJ Digit Med. 2021;4:137.
- Oppenheier J, Mandegaran R, Staabs F, et al. Remote expert DVT triaging of novice-user compression sonography with AI-guidance. Ann Vasc Surg 2023. In press.

