July/August Issue of Vein Specialist
On the Order and Timing of Venous Interventions

Sheila N. Blumberg, MD, MS
Director, AVF Board of Directors
Member, AVF Program, Newsletter, and DEI Committees
Part of the art and the beauty of venous surgery is tailoring your approach to treatment for each patient who seemingly presents with the same problem. However, like most artistic endeavors, fierce debate and research on the “correct” approach endures. Should I perform phlebectomy at the same time as the truncal ablation to avoid painful thrombophlebitis? Or should I stage the phlebectomy to minimize procedural pain, time, and potentially the number of stabs after ablation? Worse still, if there is iliac vein compression, should I treat that before I perform the ablation? Will the patient suffer a catastrophic DVT if I don’t treat this first? Essentially the same questions I had even as a trainee still have no clear answer, but each practitioner has their camp and defends it with the honor and rigor of a matador.
On one side of the bullring, you have the “always simultaneous phlebectomy with ablation” camp. The bulk of their experience has taught them that if they wait to do the phlebectomy, especially in those patients with large varicose veins, the risk of thrombosis of these varicosities and subsequent patient pain and discomfort, and now necessary delay in removing them, is not worth the risk. After all, most patients come in wanting those uncomfortable and unsightly veins gone, and now they feel worse off. Quel horreur. All it takes is one unhappy customer to validate this. Alternatively, on the other side of the bullring, the “always stage your phlebectomy” camp, they will opine that they have never seen this complication happen, and most of their patients have regression of some of their varicosities rendering the phlebectomy easier, with fewer stabs and happier patients. A less trivial question on the choice to stent or ablate first in patients with multilevel disease has vexed our community with the implied risk of a venous thromboembolic event. In the “stent first always,” they implore us that it is the safest approach to avoid a potentially catastrophic VTE. Some go even further to suggest it will improve the venous hemodynamics enough that additional ablation may not be required to achieve symptom relief. The “ablate first always” will parry that the risk of a VTE is extremely low, and in fact, they have never seen one before and perhaps ablation will also obviate the need for stenting : a much more invasive approach, involving a permanent implant! Quel horreur. To paraphrase our former president, there are fine people on both sides. But most importantly: what do most patients think and how do they actually do by-and-large with either approach? Serious intellectual rigor has gone into attempting to figure this out and the anti-climactic conclusion thus far; they do just fine. Olé!
Consensus Emerges:
Drop the Term “Accessory” for the Anterior Saphenous Vein

Edward M Boyle, MD
Founder and Director
Inovia Vein Specialty Centers
Bend, Oregon

Antonios Gasparis, MD
System Chief for Venous Diseases
Northwell Health
Greenlawn, NY

Mark Meissner, MD
Professor of Surgery, Division of Vascular Surgery
University of Washington Medical Center
Seattle, Washington
The American Venous Forum (AVF), the American Vein and Lymphatic Society (AVLS), and the Union International of Phlebology (UIP) have endorsed the findings of an international consensus panel convened to address the terminology surrounding the anterior accessory saphenous vein (AASV). It has long been established that the great saphenous vein (GSV) and small saphenous vein (SSV) are truncal veins given their envelopment in their own fascial compartment. There has remained, however, confusion surrounding the term “anterior accessory saphenous vein,” resulting in misconceptions regarding its anatomy, clinical significance, and treatment implications. The term “accessory”’ has perpetuated this misunderstanding about the true nature of this vein and its clinical relevance. This is because accessory implies it is a branch of the GSV and not a true truncal vein in its own right.
Unfortunately, this lack of clarity has significant implications for patient treatment and long-term outcomes following intervention. For example, if the anterior accessory saphenous vein is mistakenly considered a branch tributary vein, the need for treatment could be overlooked or the type of treatment provided could be inadequate, leading to the incomplete resolution of the symptoms that led the patient to seek treatment. Further, this can lead to denied payer coverage, also resulting in the same undesirable outcomes for patients. Properly identifying the vein’s role as a truncal vein is essential in developing an appropriately targeted and effective treatment plan to optimize long-term outcomes.
This has implications for many patients suffering from chronic venous insufficiency as more than 1 in 5 patients initially presenting for the treatment of superficial venous insufficiency have ASV reflux. Additionally, the ASV is becoming the most common source of recurrence in patients who have had prior GSV reflux ablation.
The panel considered that it has long been convention in both the terminology literature (which is established by clinicians) and the nomenclature literature (which is established by anatomists) that truncal veins are those enclosed within fascial saphenous compartments that drain extra fascial tributaries and are often the origin of tributary reflux. In contrast, tributary veins are not enclosed in a fascial envelope and drain into truncal veins from the subcutaneous venous network. As part of this collaboration, Alberto Caggiati, MD, Professor of Anatomy at the University La Sapienza in Rome, led the review of the anatomical considerations, advocating that the ASV should be recognized as a truncal vein and not a branch tributary given its clear and distinct envelopment in its own fascia in the upper leg.
From this process the panel unanimously suggest the name of the vein be changed from Anterior Accessory Saphenous Vein (AASV) to Anterior Saphenous Vein (ASV) to more accurately reflect its anatomic features and clinical importance. This collaboration culminated in the simultaneous publication of a series of four manuscripts in Phlebology and the Journal of Vascular Surgery: Venous and Lymphatic Disorders that were endorsed by the sponsoring societies. These publications delve into the anatomy, a systematic review of the literature, evaluation of current payer policies, and explore treatment considerations pertinent to the anterior saphenous vein.
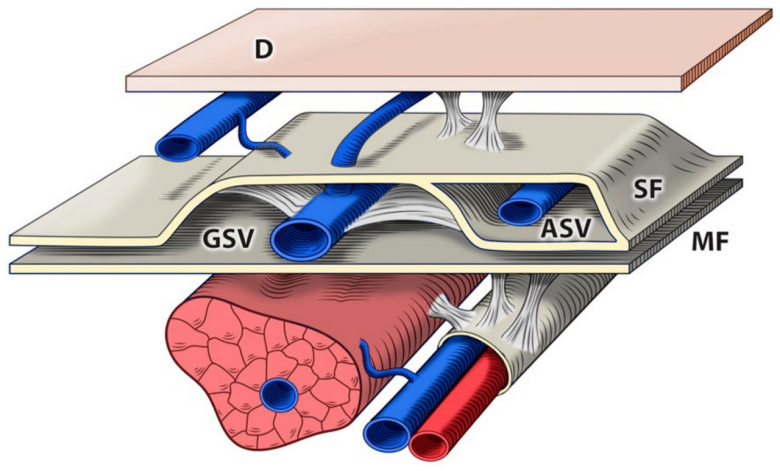
Figure 1: The saphenous compartment. D: dermis. MF: muscular fascia. SF: saphenous fascia. GSV: great saphenous vein. ASV: anterior saphenous vein.
https://www.jvsvenous.org/article/S2213-333X(24)00145-8/fulltext


Endovascular Procedures Should Be Conducted in the Office –Or Should They?

Sean Rahman
Drexel University

Swetha Sriramoju
Rowan-Virtua

Anil Hingorani, MD
NYU Langone Brooklyn
In the last two decades there has been a transition in performing vascular procedures from an inpatient setting to an outpatient setting. This largely has been based on venous procedures transitioning from open to minimally invasive procedures. This endovenous revolution started with radiofrequency obliteration of the great saphenous vein, followed by EVLA and the present era of non-tumescent nonthermal technology. Recently, the cost of venous procedures has increased and procedure revenue has decreased, while the income for vascular surgeons practicing in an outpatient setting has remained relatively unchanged.1 This has affected practitioners in the outpatient setting who are struggling financially to support their practice’s revenue and quality of care.1 As a result of the challenges faced by vascular surgeons practicing in outpatient settings, practices are closing or being bought out by hospital systems and large companies.
Alternative approaches to support outpatient practice revenue and enhance the quality of care are being explored to address financial circumstances faced by practitioners. Marketing strategies and developing a brand for practices can promote the services offered by practitioners.
Office- based labs (OBLs) must have a highly trained staff to tend to patient needs, offer a smoother service, and ensure patients return, which allows an office to grow over time.2
OBLs can demonstrate the level of care they provide by establishing accreditation from organizations including the Intersocietal Accreditation Commission (IAC), American College of Surgeons (ACS), and the Society for Vascular Surgery (SVS).3,4 Accreditation not only demonstrates a commitment to quality and safety, but offers a key competitive edge. OBLs may consider introducing various procedures including sclerotherapy, IVC filter placement, and cosmetic procedures. In addition to providing treatments for the lower extremity, OBL should consider introducing laser therapy on the face and upper extremity alongside bread-and-butter venous procedures.
Recognized as a first-line treatment for CVD, endovenous ablation procedures offer patients a faster recovery period and have been shown to be safe when conducted in an OBL.5 Iliac vein stenting is another procedure that has been concluded to be safe when conducted in the OBLs.6 Ambulatory phlebectomy is a minimally invasive procedure for treating varicose veins and improve patient care with a quick recovery period, offering another avenue for OBLs to treat patients.7 In comparison, mechanical thrombectomy, although effective in the treatment of DVTs, cannot be conducted in the OBL because the cost of the procedure and devices are prohibitive and the support needed is not readily available in the OBL.8

Krishna Jain et al. noted the challenges that vascular surgeons face with regard to decline in reimbursements following the Deficit Reduction Act of 2005, competition from other specialties, and the high cost of conducting procedures in the hospital.2 Thought to be the solution, OBLs are now facing unique and unfavorable circumstances. In sight of the challenges faced by practitioners working in outpatient settings, it is crucial to consider different paths to financially support practice revenue and enhance quality of care to sustain OBLs.
References
- Medicare physician payment on the decline: It’s not your imagination. American College of Surgeons. Updated September 1, 2019. Accessed July 3, 2024. https://www.facs.org/for-medical-professionals/news-publications/news-and-articles/bulletin/2019/09/medicare-physician-payment-on-the-decline-its-not-your-imagination/
- Jain KM, Munn J, Rummel M, Vaddineni S, Longton C. Future of vascular surgery is in the office. J Vasc Surg. 2010;51(2):509-514. doi:10.1016/j.jvs.2009.09.056
- Vascular Verification Program. American College of Surgeons. Updated January 25, 2024. Accessed July 1, 2024. http://www.facs.org/quality-programs/accreditation-and-verification/vascular-verification/
- Vascular Interventional Accreditation. Intersocietal Accreditation Commission. Updated May 1, 2024. Accessed July 1, 2024. https://intersocietal.org/programs/vascular-interventional/
- Kibrik P, Chait J, Arustamyan M, et al. Safety and efficacy of endovenous ablations in octogenarians, nonagenarians, and centenarians. J Vasc Surg Venous Lymphat Disord. 2020;8(1):95-99. doi:10.1016/j.jvsv.2019.05.011
- Satwah I, Sulakvelidze L, Tran M, et al. Iliac vein stenting is safe when performed in an office based laboratory setting. J Vasc Surg Venous Lymphat Disord. 2022;10(1)60-7.
- Andrews RH, Dixon RG. Ambulatory phlebectomy and sclerotherapy as tools for the treatment of varicose veins and telangiectasias. Semin Intervent Radiol. 2021;38(2):160-166. doi:10.1055/s-0041-1727151
- Shaikh A, Zybulewski A, Paulisin J, et al. Six-month outcomes of mechanical thrombectomy for treating deep vein thrombosis: analysis from the 500-patient CLOUT registry.Cardiovasc Intervent Radio 2023;46(11):1571-80.
